Forty-eight hours to make AI feedback feel trustworthy.
An AI-powered clinical assessment platform that gives medical students instant, structured feedback on their SOAP notes — and gives instructors actionable analytics without the grading marathon.
The problem, the solution
01 — At a glanceMedical students spend hours writing SOAP notes with little to no structured feedback. Instructors are buried under hundreds of submissions with no scalable way to evaluate them consistently. MedScor AI bridges that gap.
Medical students receive minimal, inconsistent feedback on their clinical documentation skills. Instructors lack the time and tools to provide meaningful assessments at scale — creating a critical gap in clinical training quality.
MedScor AI uses AWS Bedrock to automatically evaluate SOAP notes against clinical rubrics, delivering instant structured feedback to students and real-time progress analytics to instructors — all within a clean, focused interface.
Lead Product Designer — end to end
02 — My roleIn 48 hours, I owned the full design process — from understanding the clinical workflow to shipping a production-ready prototype that our team presented to judges.
Research
Identified user needs through rapid stakeholder interviews with a medical student and a clinical instructor within the first 4 hours.
UX Design
Mapped two complete user flows — student submission & review, and instructor dashboard — then wireframed each screen.
Visual Design
Developed the full visual language — colors, type, components — ensuring the clinical-grade feel while keeping cognitive load low.
Prototyping
Built a fully linked Figma prototype that demonstrated both flows interactively for the judging panel presentation.
Dev Handoff
Collaborated with engineers on API integration points, defining how AI-generated feedback would surface in the UI.
Presentation
Co-presented the product vision and design rationale to a panel of judges, communicating the clinical impact story.
A broken loop in clinical education
03 — The challengeMedical education relies heavily on SOAP notes — structured clinical documentation that students write to demonstrate diagnostic reasoning. But the feedback loop is broken on both ends.
Students write dozens of SOAP notes per rotation with generic or delayed feedback, making it impossible to course-correct in time. Instructors receive hundreds of submissions and can only review a fraction meaningfully.
"How might we give medical students immediate, rubric-based feedback on their SOAP notes — while giving instructors visibility into class-wide performance patterns — without adding to anyone's workload?"
Both groups wanted the same thing — signal over noise. Students wanted to know specifically what was missing or wrong. Instructors wanted to see who was struggling with what, at a glance, without reading every submission.
Two users, one system
04 — PersonasThe platform needed to serve fundamentally different mental models — a learner seeking growth signals and an educator seeking accountability data. Both needed clarity, just in different forms.

Sarah Williams
3rd Year Medical StudentJuggling rotations, studying for Step 2, and writing SOAP notes for every patient encounter. Motivated but often unsure if her documentation is meeting clinical expectations.
- Understand exactly where her SOAP notes fall short
- Get feedback immediately after submission, not weeks later
- Track improvement across multiple submissions over time
- Build confidence before entering clinical practice
- "I don't know if I'm improving or just repeating the same mistakes"
- Feedback is too vague — "good structure" doesn't help her improve
- Long wait times mean she's moved on to new cases by the time she gets a review

Dr. Michael Chen
Clinical Instructor, Internal MedicineManaging patient care alongside teaching responsibilities. Has 24 students this rotation, each submitting 3–5 SOAP notes per week. Cares deeply about student growth but can't give everyone equal attention.
- Identify which students are struggling before it's too late in the rotation
- See class-wide patterns to adjust teaching emphasis
- Reduce time spent on administrative grading
- Ensure consistent rubric application across all students
- "I have 120 SOAP notes to review this week. I can't give every one real attention."
- No visibility into who's consistently missing the same clinical reasoning step
- Grading is inconsistent — different instructors apply the rubric differently
From submission to clarity
05 — Student flowThe student experience is built around a single premise: the feedback should feel like a conversation with a knowledgeable mentor, not a grading system. Every step is designed to minimize friction and maximize learning signal.
Log In & Select Case
Students authenticate and see their active cases listed with rotation context. Each case shows the patient scenario, submission status, and deadline. Clean dashboard — no noise, just the work ahead.
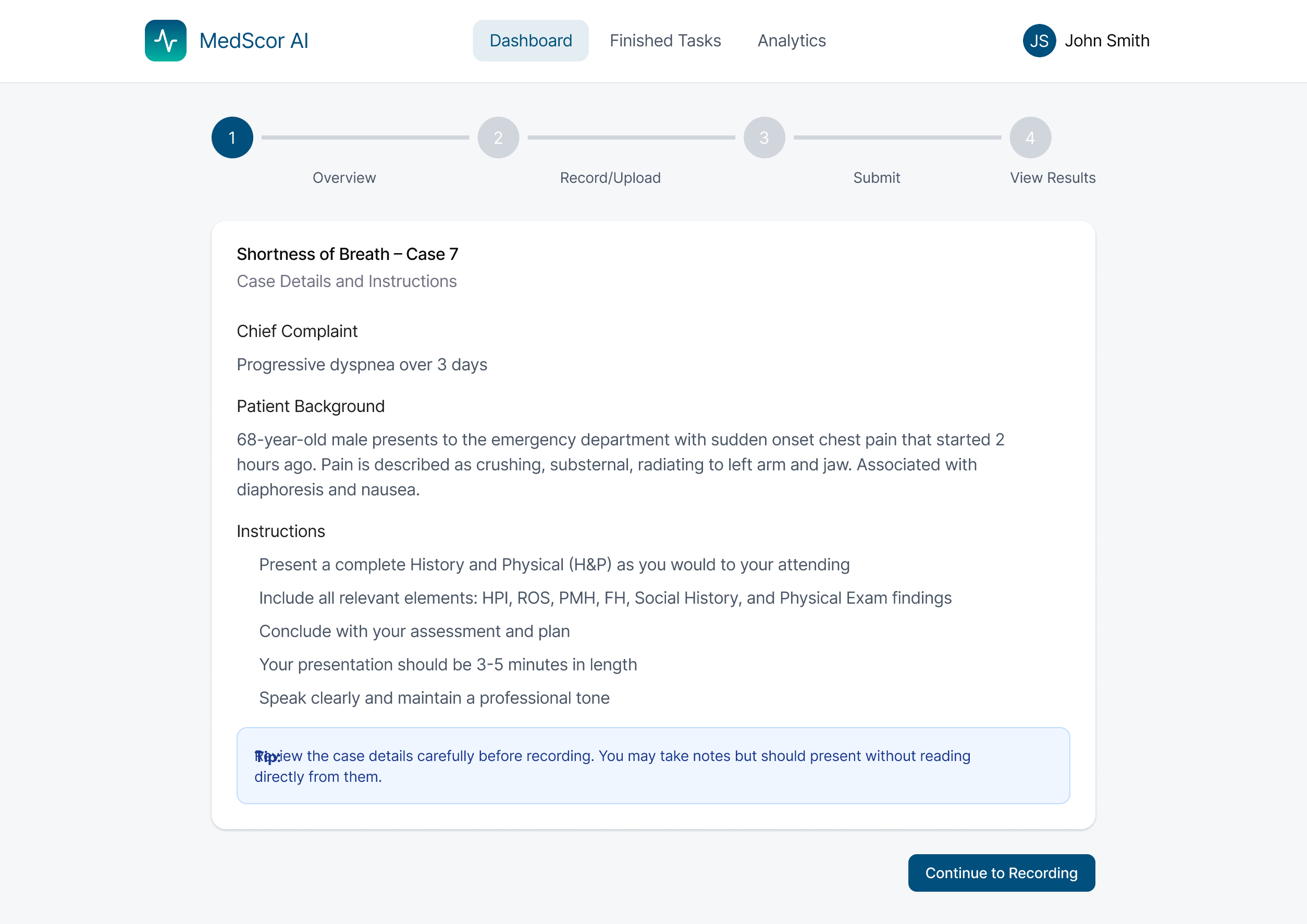
DashboardWrite SOAP Note
A structured editor guides students through each SOAP section (Subjective, Objective, Assessment, Plan) with contextual hints. The interface keeps the student in flow — no distracting notifications or complexity.
Structured EditorSubmit for AI Review
One-click submission triggers the AWS Bedrock analysis pipeline. A subtle loading state reassures the student that something meaningful is happening — not just a spinner but a brief explanation of what's being evaluated.
AWS BedrockReceive Structured Feedback
Feedback arrives instantly, broken into the rubric dimensions: Clinical Reasoning, Documentation Completeness, Diagnostic Accuracy, and Plan Quality. Each dimension gets a score and specific, actionable suggestions — not generic commentary.
AI FeedbackTrack Progress Over Time
A personal progress dashboard shows performance trends across submissions, highlighting which areas are improving and which still need work. Students can revisit past submissions with their original feedback intact.
AnalyticsTeaching at scale
06 — Instructor flowThe instructor experience is built around aggregation and exception handling. The goal: let the AI handle the volume so the instructor can focus human attention where it has the highest impact.
Class Dashboard Overview
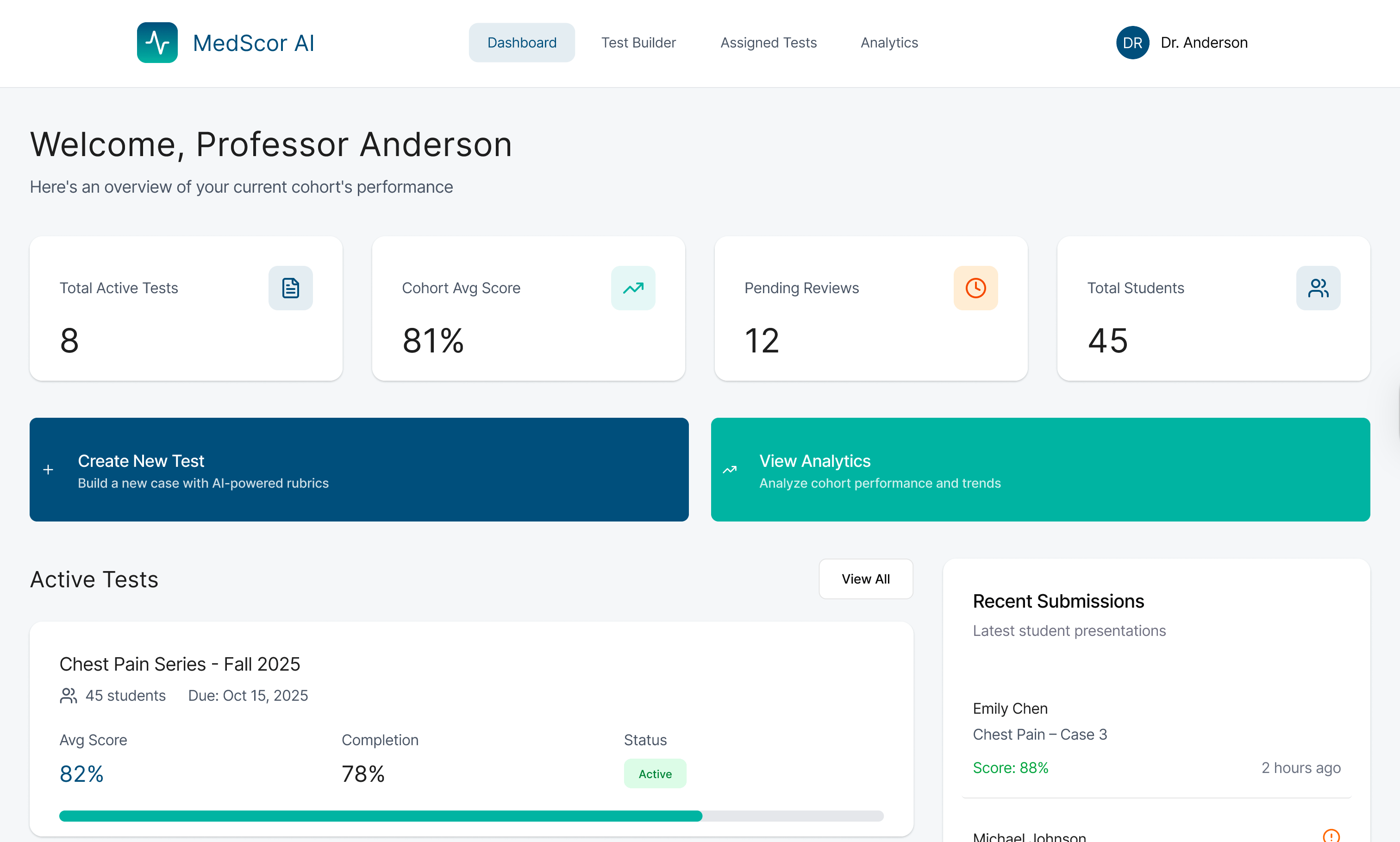
Instructors land on a class-wide view showing aggregate performance across all rubric dimensions. At-a-glance cards surface the most critical information: average scores, submission rates, and flagged outliers.
OverviewIdentify Students Who Need Help
The platform flags students with consistently low scores in specific dimensions — making it easy to prioritize follow-up. Instructors can filter by rubric category, rotation, or student to drill down quickly.
TriageReview Individual Submissions
When deeper review is warranted, instructors can open individual submissions with AI feedback pre-loaded. They can validate the AI assessment, add manual comments, or override the score — maintaining professional accountability.
Deep ReviewExport Reports & Insights
End-of-rotation reports can be exported for departmental records or accreditation requirements. The analytics also help instructors identify curriculum gaps — if 80% of students consistently fail the same dimension, the issue might be upstream in teaching.
ReportingClinical precision, human warmth
07 — Visual languageMedical tools often feel cold and institutional. MedScor AI needed to feel trustworthy and professional — but also approachable enough that students wouldn't feel judged by it. The design system balances clinical authority with human warmth.
Signal over noise.
Every element earns its place. Feedback is structured, not flooded. Instructors see summaries first, details on demand. Students see their score, their gaps, and their next step — nothing else.
AI as mentor, not judge.
Language and tone in the feedback system was designed to feel constructive and specific — more like a senior resident giving clinical notes than a grading algorithm spitting out numbers.
Trust through transparency.
Instructors can always see the AI's reasoning and override it. The system is designed to augment professional judgment, not replace it.
The final screens
08 — Final design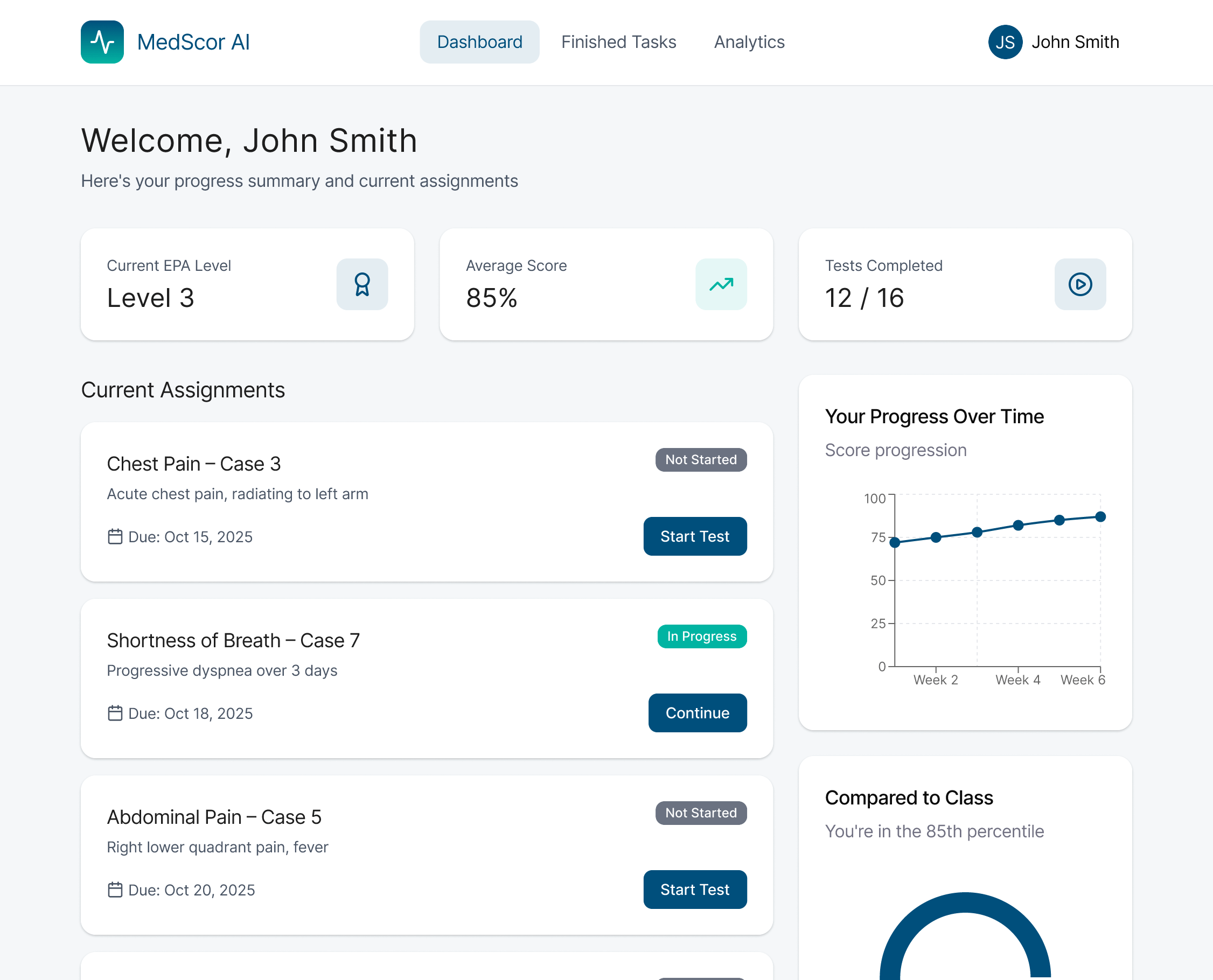
What's shipped, what's next
09 — StatusMedScor AI was built as a hackathon prototype, but the validation we received from judges and clinical educators has opened conversations about taking it further. Here's where things stand.
Completed (Hackathon)
- Full student SOAP note submission flow (5 screens)
- AI feedback display with rubric breakdown
- Instructor class dashboard with aggregate analytics
- Individual student review interface
- AWS Bedrock integration for note evaluation
- Fully interactive Figma prototype
- Design system with 20+ components
Future Development
- Real user testing with actual medical students
- Rubric customization by institution and specialty
- Mobile-responsive design for on-ward use
- LMS integration (Canvas, Blackboard)
- Longitudinal tracking across full clinical year
- Accessibility audit (WCAG 2.1 AA)
- Institutional pilot program with Rutgers medical school
Two clinical instructors who saw the demo during judging reached out afterward asking about piloting the platform in their rotations. That's the kind of feedback that tells you the problem framing was right.
What I learned building fast
10 — Reflection48 hours forces brutal prioritization. Every design decision had to be justified in seconds, not hours. Here are the three biggest takeaways from this project.
Constraints are creative fuel
Having 48 hours forced me to strip the design to its essential value proposition. Every feature I cut made the remaining features sharper. The constraint of time taught me more about prioritization than any design sprint methodology.
Domain knowledge changes everything
The first two hours were spent learning what SOAP notes actually are and how clinical instructors evaluate them. Without that grounding, I would have built a generic feedback UI. Domain research — even at hackathon speed — is non-negotiable.
AI features need UX wrappers
The hardest design challenge wasn't the UI — it was figuring out how to present AI-generated feedback in a way that felt authoritative but not overconfident. The override mechanism for instructors was the key design insight that made the whole system trustworthy.
I would have done proper usability testing with medical students before finalizing the feedback UI. The information hierarchy for the rubric breakdown was designed based on assumptions — real users might want to see the overall score first, or the specific comment first. That question deserves an answer from real data.
The result
11 — AchievementThe judges highlighted two things: the clarity of the user flows and the way the design made the AI's role legible to non-technical medical professionals. That's the validation I'm most proud of — not the trophy, but the proof that the design communication worked.